Electronic Health Records (EHR) aim to improve and streamline data entered into each patient’s permanent healthcare file. While the concept is sound, EHR implementation can be fraught with problems. Legal transcription services help address those issues by converting provider audio notes into clear, compliant documentation that supports accuracy and minimizes risk.
In This Article, You’ll Know How:
- U.S.-based transcription companies that are HIPAA-compliant and achieve high accuracy rates offer a safer, more reliable solution to EHR documentation challenges.
- EHR implementation has faced major setbacks due to cost, compatibility, and user resistance—but legal and medical transcription services can bridge that gap by improving data accuracy.
- Using low-quality or offshore transcription providers can have deadly consequences, as shown in a case resulting in a $140 million verdict.

On the surface, the process is simple. Click, input data, click save, and your health chart is updated. Sounds easy, right? The reality is that some healthcare providers haven’t completely boarded the EHR train, and two of the primary reasons are costs and ease of use.
For starters, healthcare providers in most specialties were slow to adopt EHR technology. Throughout the 1990s, hardware and software costs were high. When prices stabilized and providers eventually installed systems, compatibility problems arose. End users grew frustrated with the issues with electronic health records and ultimately resorted to scribbling handwritten notes in a patient’s chart.
Others attempted to save a few pennies by using inferior service providers or products. Later on, we’ll highlight a civil lawsuit and judgment where a patient died of an accidental overdose.
Why? Because the hospital contracted with a transcription company using foreign subcontractors who couldn’t understand the doctor’s orders, resulting in a deadly outcome. That is why using a reputable US-based medical transcription company enhances the EHR process and should be a vital consideration for any provider with a large patient base.
EHR Implementation: A Brief History
Before we dive into the history of EHR implementation, it’s essential to explain the differences between EHRs and EMRs. The two acronyms are often used interchangeably, but the difference is critical.
| Topic | Key Points |
| EMR vs EHR | EMR stays within one provider’s office. EHR is the sharable, all-inclusive record across providers. |
| Early documentation | Providers manually entered data and shared records by mail or fax. |
| Slow adoption factors | High implementation costs, HIPAA-compliant requirements, and limited tech readiness slowed adoption. |
| Adoption statistics | By 2004, only 13 percent used EHRs. In 2009, fewer than 2 percent had comprehensive systems. By 2017, about 95 percent of hospitals and 80 percent of physician practices used certified EHRs. |
| Burnout impact | EHRs increased daily work hours and reduced physicians’ time with patients. |
| Privacy and HIPAA | HIPAA mandates strict data protection and controlled access to patient information. |
| Cybersecurity risks | Hackers use ransomware, so robust security protocols are essential to prevent unauthorized access or exposure. |
| Key security features | Access controls, authentication, encryption, audit trails, and backups. |
| HIPAA violations | Top violations continue to be tracked by HHS. |
| Ethical dilemma: data input | Providers face heavy data entry burdens and must review scribe or assistant input for accuracy. |
| AI for data entry | AI voice tools still have notable error rates due to complex medical terminology. |
| Example of error risk | Similar-sounding drugs like Xanax vs Zantac highlight the danger of small transcription mistakes. |
As healthcare continues refining documentation workflows, support services that emphasize accuracy become even more valuable, which is why many providers also look to court transcription services for dependable, high-stakes record production that mirrors the precision needed in modern medical data environments.
Timeline of the EHR Evolution
Electronic recordkeeping began to emerge in the 1960s as new technologies enabled faster, more secure sharing of medical information. Academic medical centers led adoption in the 1980s, while most smaller practices stayed with paper into the 1990s due to cost and low computer use.
Even by 2004, national EHR adoption was minimal. The major shift came in 2009 with the HITECH Act, which encouraged widespread implementation.
By 2018, most hospitals and many physician practices were using EHR systems, although issues like workflow strain, accuracy concerns, and provider burnout remain.
Transcription Services and EHR
One option for entering data into an EHR system is for practitioners to record their patient interactions and have the audio files transcribed into written format by a medical transcription company.
This is a popular approach gaining in demand across the US, and many providers also rely on deposition transcription services for the same reason: they offer the high accuracy and detail needed to convert complex spoken information into reliable written records. This same precision is why medicolegal transcription services have also become an essential resource, especially when clinical documentation must align with legal standards.
However, when healthcare providers choose to save money by using non-U.S.-based transcriptionists, significant problems can and usually do arise.
In 2008, a lifelong diabetic patient was admitted to a hospital to have her dialysis port cleared of a clot. After the procedure, the physician dictated her discharge summary. However, the doctors were unaware that the medical center where the procedure occurred had contracted with a transcription company that used overseas transcriptionists to save $.02 per line.
Two days later, a nurse working at the rehab center where the patient was recovering requested the patient’s transfer orders. When told that the information wasn’t yet available, the nurse decided to print the patient’s discharge summary instead of waiting for the final transcript.
The document contained several significant transcription errors undetected by the transcription company and the quality assurance specialists dedicated to reviewing the report. The doctor had ordered eight units of insulin. Unfortunately, the AI transcribing software recorded 80 units.
After being given the incorrect amount, the patient died two days later. The family filed a lawsuit against all parties, citing negligence. After a jury trial, the treatment hospital and the three transcription companies were held responsible for the $140 million in punitive damages.
That’s one reason U.S. healthcare providers should use U.S.-based transcription companies that employ or contract only U.S.-based transcriptionists with an excellent command of English and a strong understanding of medical terminology.
In addition, any medical transcription company a healthcare provider uses must understand and be HIPAA-compliant. An essential component of HIPAA compliance is restricting third-party access (including subcontractors and freelancers) from sensitive patient records.
How to Improve EHR and Eliminate The Problems with Electronic Health Records
The good news is that more healthcare providers and facilities are using the latest technology today. With changes in the healthcare landscape, almost every provider is or will be using the technology soon.
One reason for the increasing use of EHR systems is the advent of telehealth. Implementing Clinical Documentation Improvement (CDI) is one method to help providers enhance the accuracy of an EHR system.
CDI is a new healthcare administration specialty that focuses on improving how data is entered into patient medical records. Large hospitals and providers have begun using CDI, with medium and smaller facilities following closely behind.
Another way to improve EHR data entry is to stop using copy-and-paste when entering patient information. While some providers may consider the copy-paste function a time-saving strategy, its use can result in inaccurate information and inconsistent notes in a patient’s chart. The best practice for entering patient data into an EHR platform is only to enter the exact information for that particular examination.
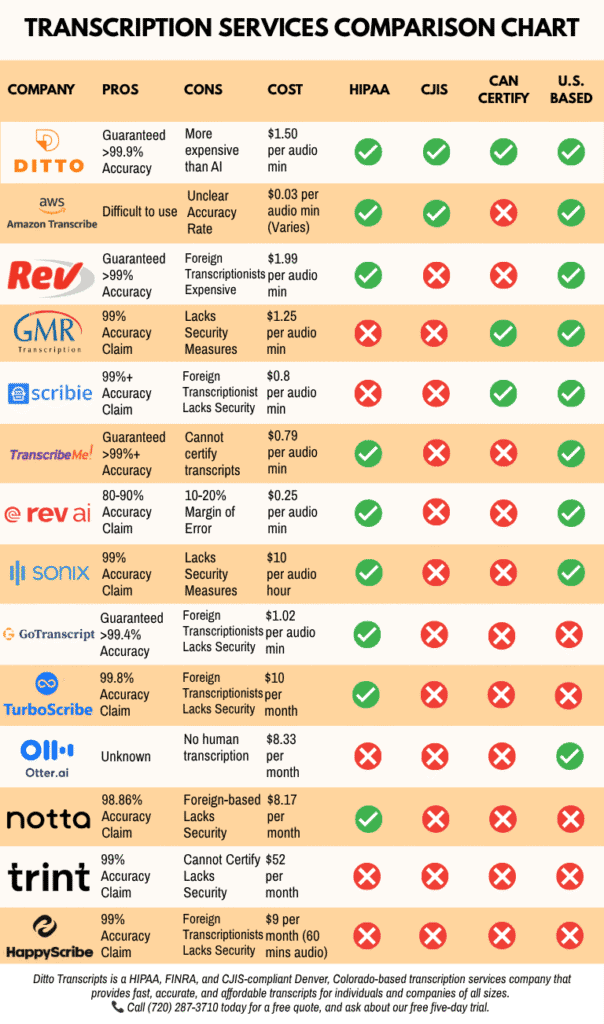
Not All Transcription Companies Are Alike
We’ve already seen the devastating adverse effects when a healthcare facility chooses a subpar medical transcription company to save two pennies per line. Let’s hope that today’s healthcare providers won’t sacrifice quality in our treatment and in the confidentiality and privacy of our personal medical records.
At Ditto Transcripts, we take pride in providing high-quality medical transcription at a competitive rate. All of our medical transcriptionists are experienced, full-time, and understand medical terminology. Plus, each medical transcriptionist we hire must have extensive industry experience and pass our rigorous testing before we onboard them.
If you need help with your electronic health records, let us know. We would be happy to help you become more efficient with it.
The best part? There’s no need to break the bank for our services. We’ll be happy to let you in the loop on our legal transcription prices. If that does not sound convincing yet, here’s what our testimonials look like:

Ditto Transcripts is a Denver, Colorado-based FINRA, HIPAA, and CJIS-compliant transcription services company that provides fast, accurate, and affordable transcripts for individuals and companies of all sizes. Call (720) 287-3710 today for a free quote.